
It's as easy as ordering a book online: Sign up for an account, choose a method of payment, and receive the package in three to four business days.
But first, there are some choices to make. The fentanyl hydrochloride comes in a variety of quantities, ranging from a half-gram sample for $35 (U.S) to a kilogram for $21,000. It also comes in different strengths – purchasers are warned to "be careful" and do their research on the product, described as 99-per-cent pure. And of course, there are the related pharmaceutical products: the fentanyl patches, tablets and even lollipops.
Buyers are assured their package won't get seized at the Canadian border. To avoid the risk of detection, says a supplier from China, he conceals the purchase alongside urine test strips. Not that there's reason to worry: Canadian border guards cannot open packages weighing less than 30 grams without the consent of the recipient. (A Globe and Mail reporter corresponded with sellers and suppliers using a pseudonym and did not disclose himself as a journalist, in order to obtain accurate information from the seller.)
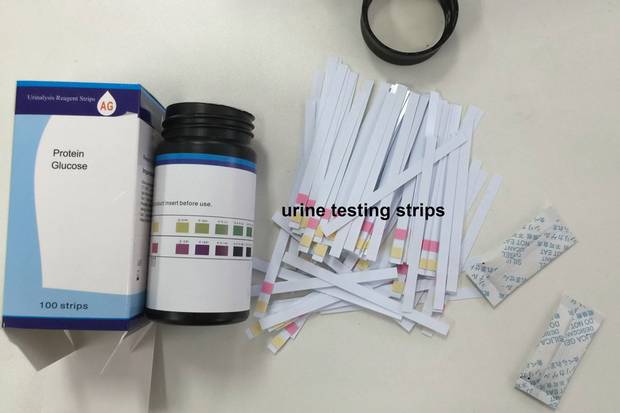
Suppliers in China hide fentanyl in decoy packages before shipping the drug to Canada. Sometimes they conceal the drug alongside urine test strips.
The supplier, who identified himself only as Alan, says he has two customers in Canada. He e-mails photos of fentanyl hidden inside silica-desiccant packets – the type normally used when shipping goods such as electronics – and a screen shot of a recent order from Canada, including a shipping address for a clothing store in British Columbia's picturesque Okanagan Valley.

Fentanyl from China is sometimes hidden in silica desiccant packages.
Alan says he is based in the southern metropolis of Guangzhou, the trading crossroads for manufacturing in China – a country that is, in turn, at the centre of the vast underground world of synthetic-drug manufacturers. Enforcement is fragmented, and companies operate with impunity.
Fentanyl is an opioid, a class of painkillers that also includes oxycodone and morphine. Prescription-grade fentanyl is up to 100 times more toxic than morphine. Developed in 1959 by a Belgian chemist, it was quickly adopted as a pain reliever and anesthetic in medical settings. It came into widespread use in the mid-1990s with the introduction of the transdermal patch that releases the drug into the patient's bloodstream over two or three days. When the drug is processed in a clandestine lab with no quality controls, it is difficult to get the dosage right, making it potentially much more dangerous.
Chemical companies in China custom-design variants of pharmaceutical-grade fentanyl by tweaking a molecule ever so slightly. A few hundred micrograms – the weight of a single grain of salt – are enough to trigger heroin-like bliss. But the line between euphoria and fatal overdose is frighteningly thin: An amount the size of two grains of salt can kill a healthy adult.
The supply chain for illicit fentanyl begins in China, but the problems Canada is experiencing start right here at home: No other country in the world consumes more prescription opioids on a per-capita basis, according to a recent United Nations report. The widespread use of prescription opioids is behind the rise of a new class of drug addicts, many of whom are turning to the black market to feed their habit. In British Columbia and Alberta, the two hardest-hit provinces, fatal overdoses linked to fentanyl soared from 42 in 2012 to 418 in 2015.
A Globe investigation has found that many of those deaths could have been avoided.
Among the investigation's findings from interviews with nearly three dozen medical experts, public-health doctors, police and family members of overdose victims: Federal and provincial rejection of harm-reduction measures hindered the response to the fentanyl crisis in Alberta. Neither Ottawa nor the provinces are taking adequate steps to stop doctors from indiscriminately prescribing highly addictive opioids to treat chronic pain – in 2015 alone, doctors wrote enough prescriptions for one in every two Canadians. And addiction-treatment programs are few and far between – a legacy of the former Conservative government's tough-on-crime policies.
The investigation also found that online suppliers are exploiting gaps at the border. Fentanyl and many chemically similar drugs are classified as controlled substances in Canada, making them illegal to import without a licence or permit. But, for online suppliers, the borders may as well not exist; they devise clever ways to conceal the drugs and skirt inspection rules. Suppliers often ship drugs in packages under the 30-gram threshold, ensuring border agents won't open them. One supplier with whom a Globe reporter corresponded promised to ship fentanyl inside a gift-wrapped package. Another pledged, "No problem of police coming to you," as the package would be labelled household detergent, complete with a certificate of analysis. Many suppliers will even offer guaranteed reshipment to customers in the event their package gets intercepted.

Because illicit fentanyl is so potent, once it arrives here, the white crystalline powder gets diluted with powdered sugar, baby powder or antihistamines before it can be sold on the street and consumed. It is also mixed into other drugs, and sold as heroin or OxyContin.
As Canada wakes up to a mounting public-health crisis, it is left playing catch-up with the United States, which is confronting its own epidemic of illicit and prescription drug abuse. Policymakers in Canada do not even have the basic tools to monitor this leading cause of accidental deaths – in contrast to the situation in the United States, there is no national system tracking fatal opioid overdoses.
The arrival of illicit fentanyl in Canada is a "game changer," says Benedikt Fischer, a senior scientist at Toronto's Centre for Addiction and Mental Health. When Canada's opioid problem involved only the abuse of prescription drugs, he says, policymakers squandered an opportunity to address it. Now that many addicts are turning to a drug that is manufactured without government oversight – and in countries beyond our borders, to boot – it is nearly impossible to get a grip on the problem. "Even if we wanted to now suddenly take action, there's nothing we can do," he says. "We have no way of controlling thousands of illegal drug labs in China."

Jason Berry (left) and Patrick Provencher were arrested in 2013 for producing and distributing fentanyl tablets. It was the first big Canadian fentanyl bust.
Handout photo
An unprecedented drug bust
It was the winter of 2012 when a Montreal police detective heard about a drug-dealing operation run by local gym rat Patrick Provencher, who was, at the time, unknown to police. But it would take another year for Det. Yves Rousseau to confirm the seemingly innocuous tip about the low-level drug dealer – one that would lead to the first big bust of a Canadian operation dedicated to producing and selling industrial quantities of bootleg fentanyl.
The case was uncharted territory for Canadian law enforcement – three investigators became ill after kicking in the door of the illicit lab and handling the toxic drug, including one who spent a night in hospital. The police drug lab, to which hundreds of kilograms of drug-making substances were hauled, was placed under quarantine. The fire department's hazardous-material unit had to decontaminate the drugs before they could be examined.
"All of these products were in residential neighbourhoods, next to people living their lives," Det. Rousseau testified in court proceedings, after Mr. Provencher's 2013 arrest, as he told an astonished judge about the turn of events. "This was very dangerous to public security."
About a year after police were tipped off about Mr. Provencher, a 40-year-old computer engineer trained at Montreal's École Polytechnique, a second source confirmed the information – and added more: Mr. Provencher had recruited Jason Berry, a 33-year-old who had just served time for producing and selling drugs, as his business partner. The two men had set up a lab in a garage in the hardscrabble Pointe-Saint-Charles neighbourhood, rented several storage units, and were running the business out of the downtown gym where Mr. Provencher worked.
They received raw material from China, cut the drug with fillers, put the mixture through a pill-press machine to produce tablets, and then shipped them by courier all over North America, often in hollowed-out appliances. In fact, police arrested the two men on their way to a UPS store to ship a microwave oven containing 10,180 fentanyl tablets to New Jersey.
Police found nearly 200,000 pills in various storage units along with pill presses, pulverizers and dryers capable of churning out thousands of tablets an hour. The two men pleaded guilty, and were each sentenced to about eight years in prison in 2014, minus credit for time served.
"The quality of the pills was unbelievable and the quantity was unheard of," Det. Rousseau said.

Purdue began sending adverse drug reaction reports to Health Canada in 2000, describing everything from patients who experienced hot and cold sweats and dizziness after taking Oxycontin to fatal overdoses, according to documents obtained by The Globe through an access to information request.
Opioid nation
The raid of the Montreal lab in April, 2013, shows how fentanyl has revolutionized the illegal drug trade. Unlike the massive infrastructure and cartels required to manufacture and transport heroin or cocaine, just about anyone can buy and sell fentanyl. Because it is so powerful, a little goes a long way. A kilogram ordered over the Internet – an amount equal in weight to a medium-sized cantaloupe – sells on the street in Calgary for $20-million, making it a drug dealer's dream.
The collective inaction of government leaders, doctors, police and border officials leaves Canada dealing with the fallout from a drug that wouldn't even be on the streets were it not for a decision made two decades ago. Until the mid-1990s, opioids were primarily prescribed to cancer patients and others suffering debilitating pain. But in 1996, Health Canada approved OxyContin, a brand-name version of oxycodone, to relieve moderate-to-severe pain, heralding a sea change in the treatment of pain.
Purdue Pharmaceutical, the maker of OxyContin, launched sales campaigns promoting the benefits of the drug. Doctors started prescribing it for everything from backaches to fibromyalgia. OxyContin quickly became the top-selling long-acting opioid in Canada. But it also became a lightning rod in the early 2000s, as reports of addiction and overdoses exploded.
The Office of the Chief Coroner of Ontario raised concerns, noting in a 2004 report that deaths linked to oxycodone climbed steadily between 1999 and 2003, according to documents obtained by The Globe through an access-to-information request. The report says that although no attempt was made to determine whether the detected oxycodone was due to "the ingestion of OxyContin or any other oxycodone-containing formulation, it is noteworthy that the increase in the prevalence of oxycodone findings in death investigations coincides with the introduction of Oxycontin [sic] to the Canadian market."

OxyContin was popular not only with people who became addicted after receiving prescriptions, but also with heroin users, because they could easily snort it like cocaine or inject it like heroin for a quick high.
In 2012, Purdue pulled OxyContin from the market and replaced it with OxyNEO, a tamper-resistant alternative that is difficult to crush, snort or inject. That same year, the provinces stopped paying for either opioid through their public drug plans. But by focusing specifically on those two drugs, medical experts say, policy makers missed the larger picture. Prescriptions for alternative painkillers, including hydromorphone and fentanyl, rose sharply: The crackdown pushed drug abusers and legitimate patients towards other, potentially addictive painkillers.
The removal of OxyContin left a void that organized crime exploited, says Sgt. Luc Chicoine, the RCMP's National Drug Program Co-ordinator. Responding to an e-mail from The Globe, Purdue spokeswoman Aimee Sulliman said that the increase in fentanyl-related deaths across Canada is "tragic and a significant public-health concern," but that it is unfair to blame OxyContin for the rise of the illicit drug. "This is a complex issue and the simplistic causality assertion of the question is misleading."
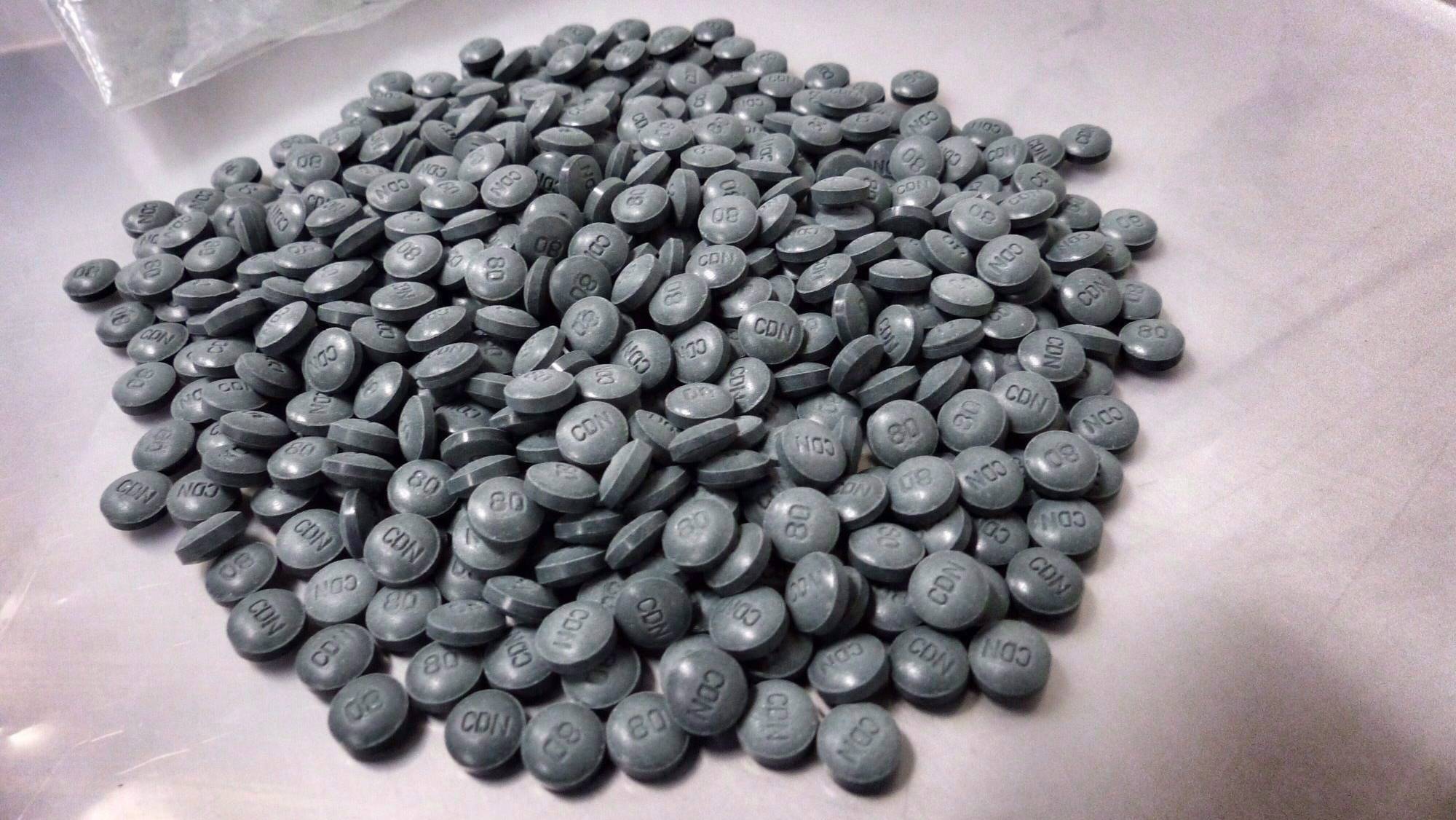
Demand for a replacement for OxyContin also gave rise to another problem – a counterfeit version of the drug laced with illicit fentanyl smuggled into Canada and processed for street sale in labs. The labs would typically dye their pills green to mimic the 80-milligram OxyContin pills favoured by opioid abusers, and sell them as "greenies" or "shady eighties."

Fentanyl pills are made to look similar to OxyContin pills.
Alberta Law Enforcement Response
In comparison to Europeans, North Americans rely heavily on pharmacological solutions to medical woes. In a culture whose citizens pop over-the-counter pills to treat every minor ailment, says Sgt. Darin Sheppard, of the RCMP's Federal Serious and Organized Crime Synthetic Drug Operations, many drug users view the "greenies" as deceptively harmless.
"It's just a pill to many people," Sgt. Sheppard says. "Now, we're starting to realize the true aspect of what harm can be realized as a result of this."
Police across Canada have shut down 20 fentanyl labs since that first major bust in April, 2013, mostly operated by organized-crime groups, according to a Globe review. The biggest raids were in B.C., Alberta and Saskatchewan. Police have also made dozens of busts involving illicit fentanyl and the prescription-grade patches. This week, police charged a doctor and a pharmacist from the Toronto area with participating in a fentanyl trafficking ring.

The Canada Border Services Agency (CBSA), the first line of defence in preventing illicit goods from entering the country, is responsible for clearing international mail. In 2015, the agency made just under 11,000 illicit-drug seizures, half of which came through the postal system. And yet, even as the volume of all commercial goods cleared at the border increases, including international mail, the number of front-line officers continues to shrink.
As long as fentanyl continues to arrive in Canada undetected, municipal police cannot arrest themselves out of the problem, says Calgary Police Staff Sgt. Martin Schiavetta. He wants to know how serious the federal government is about fentanyl. "Are they aware of the scope of the problem?" he asks. "What strategies does the RCMP have to deal with these Chinese imports? Does CBSA have enough capacity to deal with all the packages?"
The problem is compounded by the fact that the illicit drug is highly profitable for traffickers. Hakique Virani, an Edmonton physician and former deputy medical officer at Health Canada, described the "whack-tastic" profits for traffickers during a conference last November for the Canadian Society of Addiction Medicine. The raw materials and equipment, including a kilogram of pure fentanyl powder and an industrial-grade pill press, cost under $100,000, he said in his presentation. A kilo of powder is enough to produce one million tablets, which sell for $20 each in Calgary. Police chiefs in Alberta asked the federal government last November to make it illegal to import and operate industrial pill presses, but have had no response.

Injection stalls at Insite, the legal supervised drug injection site, in Vancouver, B.C. on Friday July 17, 2015.
Rafal Gerszak For The Globe and Mail
Deadly denial
Many medical experts say that the former Conservative government did not devote enough resources to harm-reduction measures (such as the provision of overdose antidotes) to address the side effects of drug abuse; Ottawa fought a war on drugs instead, primarily by prosecuting low-level offenders.
Any mention of harm reduction was banished from Health Canada's website in 2007, when the federal department changed the name of its National Drug Strategy to the National Anti-Drug Strategy.
The Conservatives quietly spread the word that not-for-profit groups would have difficulty getting federal funding if they continued to provide harm-reduction programs. Margaret Ormond, project director of Sunshine House, a harm-reduction centre in Winnipeg, says she was told that if she wanted to continue receiving funding from Ottawa, she should not "go on and on about harm reduction" in her application. Sunshine House stopped seeking federal funding six years ago.
Stephen Harper's Conservatives also attempted to shut down Insite, North America's only supervised-injection site, in Vancouver's impoverished Downtown Eastside, which allows addicts to safely inject illegal drugs under a nurse's supervision. The Conservatives eventually lost that battle at the Supreme Court of Canada, which in 2011 ordered the government to allow Insite to remain open. The government responded to the ruling by introducing legislation making it difficult, if not impossible, for other sites to open, even though Insite has demonstrated that it has reduced overdose deaths.
"Under the previous government, Health Canada did virtually nothing of consequence to address this epidemic," says David Juurlink, head of clinical pharmacology and toxicology at Sunnybrook Health Sciences Centre in Toronto. "In some ways, their actions have made it worse."
Health Canada did not reply to The Globe's request for comment on how opioids are managed. In a statement, the spokesman for Alberta's health minister said that the province is actively looking for ways to improve physician education and prescription monitoring, but could not provide specifics on when any results are expected.
In an interview, federal Health Minister Jane Philpott says she is committed to addressing the problem and to making sure people struggling with opioid abuse have access to harm-reduction programs. "I have talked to families who have lost loved ones, whose lives could have been saved if they had either the opportunity to access a supervised-injection site or if the family had known about the availability of naloxone," Ms. Philpott says, referring to an antidote that reverses the symptoms of an overdose in minutes. "Nothing is more heartbreaking than hearing the stories of these families."
Rupa Patel, a family physician in Kingston – who, like a lot of her colleagues, has many patients asking for prescription opioids – sees an additional way the government could help mitigate the crisis: by introducing mandatory prescribing limits.
Unlike the United States, which released new guidelines last month advising doctors not to prescribe opioids for chronic pain in most situations, Canada has not revised its guidelines since 2010. Opioid prescriptions totalled 19.1 million in 2015, up from 18.7 million the year before, according to figures compiled for The Globe by IMS Brogan, which tracks pharmaceutical sales.
Dr. Patel sets her own limits with her patients, often refusing to prescribe painkillers, because the risks are substantial and the benefits uncertain. But saying no is difficult, she says, because patients are often in distress. "People expect a pill to fix their problems."
Even if new guidelines were introduced, there are still not enough resources, nationally, to treat addiction. More beds are needed for those going through withdrawal as well as treatment programs for people addicted to painkillers, especially for aboriginals and those living in remote areas.
And as the pipeline for black-market drugs leads to an unprecedented surge in deaths, Canada has been slow to make naloxone more widely available. Last month, Health Canada changed the status of naloxone to a non-prescription drug. But before it can be sold without a prescription, each province and territory needs to approve the loosened restrictions – something that is not expected to happen until June or July in several regions.

Standoff is a community of 12,800 people that has endured a disproportionate number of Alberta’s fentanyl deaths.
Chris Bolin For The Globe and Mail
An expanding crisis
No province has been hit as hard as Alberta, where fentanyl was found in the blood and urine of 392 fatal-overdose victims over the past two years.
During those early days of the crisis, both federal and provincial health officials were slow to grasp the enormity of the problem, The Globe investigation found. The Alberta government did not issue a province-wide warning to doctors about illicit fentanyl until December, 2014. And it was not until a year later that Alberta's health minister allowed all first responders across the province to treat overdose victims with naloxone.
The southwestern community of Stand Off, on the Blood Tribe reserve (also known as Kainai Nation), has endured a disproportionate number of Alberta's deaths. Dr. Esther Tailfeathers, a family physician from Blood Tribe, responded to her first fentanyl overdose in July, 2014. She had just pulled her car into the parking lot of a shopping centre in Lethbridge when she saw a man in a white minivan slumped over the steering wheel. Only minutes earlier he had taken a pill. In the back seat, four children were crying for help as he lost consciousness.
The young man would survive that day. But within months, the reserve in a socially conservative corner of Alberta, where neighbouring communities enforce prohibition and cherish abstinence, would become ground zero for an emerging public-health crisis.
Within days of her first brush with fentanyl, Dr. Tailfeathers began seeing other overdose victims in her hometown of 12,800. At first, she treated one or two overdose cases a week. But that quickly escalated to two or three a shift.
"We've never seen anything like this," she says.
Patients soon began sharing stories about illicit pills circulating in the streets of their sprawling reserve near the Montana border. Drug dealers from Calgary and the small First Nations community of Maskwacis travelled there with backpacks full of fentanyl, selling each pill for $80. One girl collapsed at a party after snorting fentanyl, Dr. Tailfeathers says. "We put a tube in her nose, and while she and I were talking I pulled the tube out. There was a green pill stuck in the end."
By August of 2014, reports of mounting deaths in Blood Tribe began arriving in the Edmonton office of Dr. James Talbot, the province's chief medical officer at the time. Dr. Talbot quickly set up a working group and invited Dr. Michael Trew, then the province's chief addictions and mental health officer, to join.
The first thing the two doctors tried to do was distribute naloxone kits to first responders. But they ran into roadblocks: While specialized paramedics were allowed to administer the drug, the majority of first responders in Alberta could not.
The Blood Tribe ended up reaching out to Dr. Virani, who was then still a deputy medical officer at Health Canada, for its first batch of naloxone kits. Dr. Virani remembers his employees going to discount stores to buy the plastic containers that would hold the first 90 doses of the antidote. "At the time that I sent naloxone to Blood Tribe, Health Canada made every effort not to talk publicly about it," he says.
Meanwhile, crime rates began to soar in Blood Tribe. The community was already struggling with poverty, income inequality and substance abuse. Addicts were breaking into homes looking for valuables. People sold everything they owned to buy another pill, says Dr. Tailfeathers, with some nursing a habit that cost as much as $300 a day. She visited homes where there was no food, no heat and no blankets. The four walls of one house were covered with writings about suicide. "It's like a natural disaster on the reserve," she says.

A fence is tagged with “SSB” - South Side Bloods along a street in Standoff nicknamed Oxy-Alley. Crime rates in the small community increased as fentanyl use spread.
Chris Bolin For The Globe and Mail
In March of 2015, the local band council declared a state of emergency, making it the first community in the country to sound the alarm because of fentanyl. Despite that, Dr. Virani says that Health Canada told him to stop speaking publicly about First Nations health in Alberta. He resigned from the department last month. While he declined to comment about his departure, he accused the bureaucracy of being slow to respond to the fentanyl crisis and being out of step with the minister, Dr. Philpott. "I think she's a public-health champion on this," he says.
The naloxone program that Dr. Virani started in Blood Tribe, where the federal government has jurisdiction, helped reduce the number of people overdosing. But once the epicentre of the fentanyl crisis shifted to Calgary, it was up to the provincial government to take action.
In the final months of the former Conservative government's time in power, the health minister mobilized the first resources to combat fentanyl. Shortly before the government was defeated last May, Alberta sent a notice to hospitals and clinics warning about the risks associated with illicit fentanyl and recommending naloxone to reverse the effects of an overdose. The end-of-government decision may explain what happened next. During the first chaotic week of New Democratic rule in Alberta, both Dr. Trew and Dr. Talbot were told by senior members of the civil service that they were being let go when their contracts expired. A new chief medical officer has yet to replace Dr. Talbot.
The strain was clear on Staff Sgt. Schiavetta's face during an interview in February. He took over Calgary Police's drug unit in early 2015, just as fentanyl use began to skyrocket in the city – 81 people in Calgary died from fentanyl overdoses last year, including residents of all genders, ages and socioeconomic groups. Complicating matters, his officers seized three pills last August that were later identified as W-18, an experimental drug 100 times more potent than fentanyl.
But fentanyl remains the drug that takes up most of Staff Sgt. Schiavetta's time. "Calgary is flooded with fentanyl," he says.
While Alberta has borne the brunt of the fallout from the arrival of bootleg fentanyl from China, no one saw it coming, Dr. Trew says. "It hit us between the eyes."
The scourge of illicit fentanyl is now rapidly expanding east. Deaths linked to fentanyl more than doubled to 29 in Manitoba last year, according to a Globe tally of provincial coroners' figures. In Ontario, fentanyl was the leading cause of opioid deaths for the first time in 2014 – the most recent figures available – and several communities (including Toronto, Kingston and the Niagara region) have been hit with a spike in fatal overdoses in recent weeks.

Vendors in China sent pictures of their labs to Rodney Bridge, an Australian man who became an expert on Chinese drug manufacturing after his 16-year-old son died from taking drugs.
Back to the source
Little is known about the companies in China that make fentanyl, including whether the substance is the product of backyard laboratories or professional chemists concocting it on the side. Or, more likely, both.
For most potential buyers, fentanyl manufacturers appear to exist in plain view, openly advertising the drugs they make. On the Chinese Internet – where no trace of them can be found – and on the ground, it's a different story altogether.
A Globe reporter travelled to Wuhan to search for the addresses posted online by a series of drug sellers and laboratories. One address pointed to a massive apartment-construction project. Several others were for street numbers of buildings that have either been demolished or were never there.
One clue lies in photographs sent to Rodney Bridge, an Australian man who became an expert on Chinese drug manufacturing after his 16-year-old son died from taking a lab-made drug similar to LSD. His son jumped off a balcony, thinking he could fly.
Mr. Bridge travelled twice to China in search of the person who sold the $2 pill to his son. Vendors sent him pictures of their labs. One showed a cobbled-together arrangement resembling a high-school chemistry lab. Another showed a large industrial operation in a warehouse, complete with a forklift.

A photo of a lab that a Chinese drug vendor sent to Rodney Bridge.
Chinese officials have taken steps to crack down on the illicit drug business. Last October, the country banned 116 substances, including a half-dozen types of fentanyl. Hu Minglang, a director of China's National Narcotics Control Commission, told The Globe the ban has been "very effective."
But the ban appears only to have succeeded in placing chemicals slightly under the radar. Dharma Chemicals, a supplier named by the World Health Organization as a seller of acetylfentanyl, one of the 116 illegal chemicals, has struck the drug from its catalogue. But in response to e-mailed queries from a Globe reporter, a Dharma representative promised quick delivery of the drug, writing, "stock is available."
China remains in some ways the ideal country to produce synthetic drugs, something no rules are likely to change. As the world's biggest trading nation, China already sends huge volumes of goods to countries such as Canada, providing "numerous ways to disguise your drugs," says John Coyne, a former Australian Federal Police intelligence agent who is now head of border security at the Australian Strategic Policy Institute.
It's a problem the Mexican government has combatted for years. Mexican drug cartels have long imported chemical ingredients from China, which fuel the Latin American country's manufacture of meth and finance its crime syndicates. "China was never willing to help. They didn't see it as their problem," says Jorge Guajardo, the Mexican ambassador to China from 2007 to 2013.
As long as Chinese officials do not crack down more aggressively on exporters, medical experts say, the responsibility for change falls squarely on those in power at the end of the supply chain. "It's a national tragedy," says Meldon Kahan, medical director of the Substance Use Service at Women's College Hospital in Toronto, "and a health-care tragedy where most groups don't come out looking very good."
Life lost One mother’s tragic slide into fentanyl addiction
4:11
Out of the shadows
It's also a tragedy that often plays out in private.
Many people living with substance abuse suffer in silence, all too aware that society tends to blame the victim and view opioid dependence as a character flaw. Michael Franklyn, an addiction doctor in Sudbury whose practice spans urban and rural communities throughout Northern Ontario, says that nearly one-third of the patients he treats for opioid addiction were initially prescribed the drug by their physician. But people who become addicted are often stigmatized by society, he says, even though no one ever makes a conscious decision to go down that path. "It's not a population people get excited about treating," he says.
The stigma is also felt by the loved ones of victims of fatal overdoses. A Globe reporter interviewed a couple whose 21-year-old son died just over three years ago after he overdosed on prescription-grade fentanyl purchased on the street. The couple, who asked that their names not be used, say they have not told anyone, including their parents, how their son died.
"It's our private feelings or thoughts and we don't need anybody else knowing," the mother says. "I don't want anybody to think bad of him. He was a great guy."
Their son never missed a day of work, so his father was surprised one Monday morning when he didn't wake up. When he went into his son's bedroom, he found him with no apparent vital signs. His laptop was open – the last message posted by a friend just before three in the morning, upset that he had not responded to her.
Their son had not been prescribed painkillers; he got addicted after using opioids recreationally. He was private, and determined to cope with the problem on his own. By all outward appearances, he seemed to be doing just fine. He graduated from high school, took a two-year welding course at community college, and had a full-time job at a steel company. He was social with lots of friends. His hobby was tinkering with the engine of his Oldsmobile coupe. "When we buried him," his father says, fighting back tears. "He still had grease under his fingernails."
Some parents have gone public in a conscious effort to combat the stigmatization. Petra Schulz, a lecturer at Edmonton's MacEwan University, has blogged and spoken about her son's death from a fentanyl overdose, which occurred on April 30, 2014.

Danny Schulz was 25 when he died from a fentanyl overdose on April 30, 2014.
Amber Bracken For The Globe and Mail
Ms. Schulz tried to call her son that day, but he didn't pick up the phone. While the 25-year-old had used drugs in the past, he seemed to be clean, and had returned from a long trip with his father only two days earlier. That evening, she went to his downtown apartment in Alberta's capital and let herself in. A tinny radio was playing the CBC news, a newspaper was scattered on the table, and an unopened beer was nearby.
Read: Lives Lived: Daniel (Danny) Schulz, 25
Just as she was about to leave the apartment, she noticed a light under the bathroom door. She found Danny's body behind it, on the floor.
"When you have a child who struggles with addiction, you have that fear that one day they will overdose," Ms. Schulz says. "And then I saw that light, and I didn't hear any sound from the other side of the door."
With a report from Andrea Woo in Vancouver.
Editor's Note: An earlier version of this story incorrectly stated that a fentanyl lab was busted in the Northwest Territories. This version has been corrected.